Most superficial lumps and bumps encountered in an outpatient surgical (OPD) clinic are benign. Early assessment focuses on duration, growth rate, symptoms (pain, discharge, skin changes), mobility, and systemic signs. Red flags that prompt urgent referral include rapid growth, hard/immobile mass, skin ulceration, unexplained weight loss, or regional lymphadenopathy.
1. What is a Lipoma?
Description: Benign soft fatty lump under the skin. Usually soft, mobile, painless, and slow-growing.
Typical presentation: Round/oval, soft, rubbery, mobile, most commonly on trunk, shoulders, neck.
Investigations: Clinical diagnosis; ultrasound if deep or uncertain; MRI if large or suspected liposarcoma.
Treatment options: Observation for asymptomatic lesions; elective surgical excision (minor procedure) for symptomatic or cosmetically bothersome lumps.
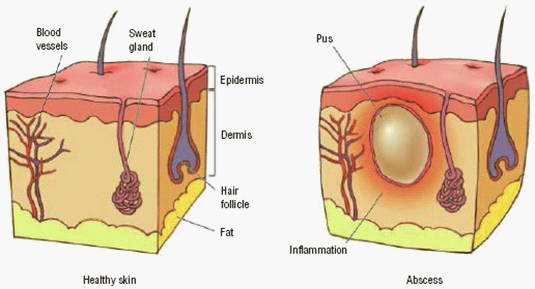
2. Epidermoid (Sebaceous) Cyst
Description: Benign cyst from blocked hair follicle or sebaceous gland; often has a central punctum.
Presentation: Firm, mobile lump with occasional intermittent discharge or inflammation if infected.
Investigations: Clinical assessment; ultrasound if deep or atypical; culture if infected.
Treatment: Incision and drainage for acute infection (temporary); elective complete excision including cyst wall to prevent recurrence once inflammation subsides.
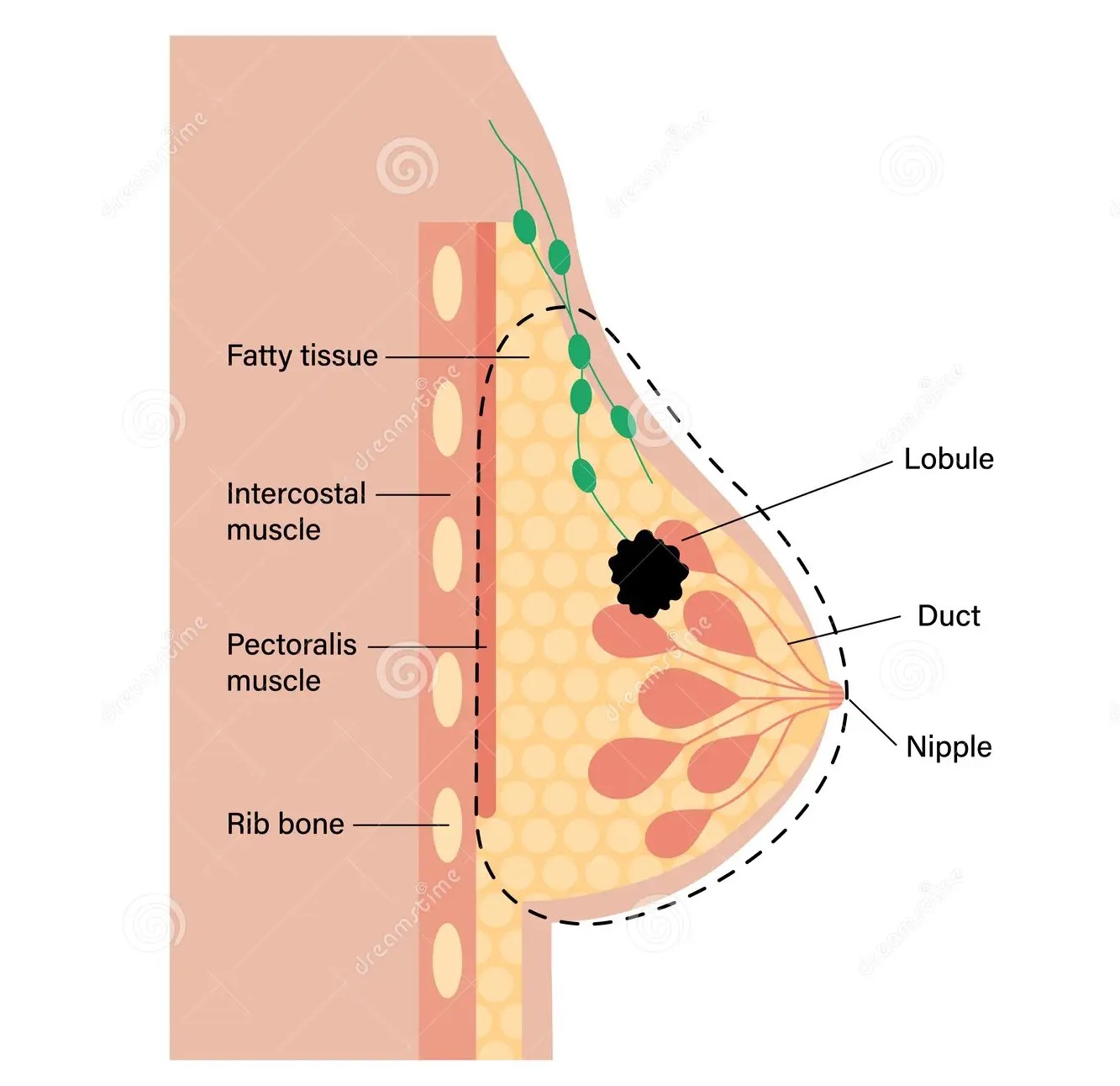
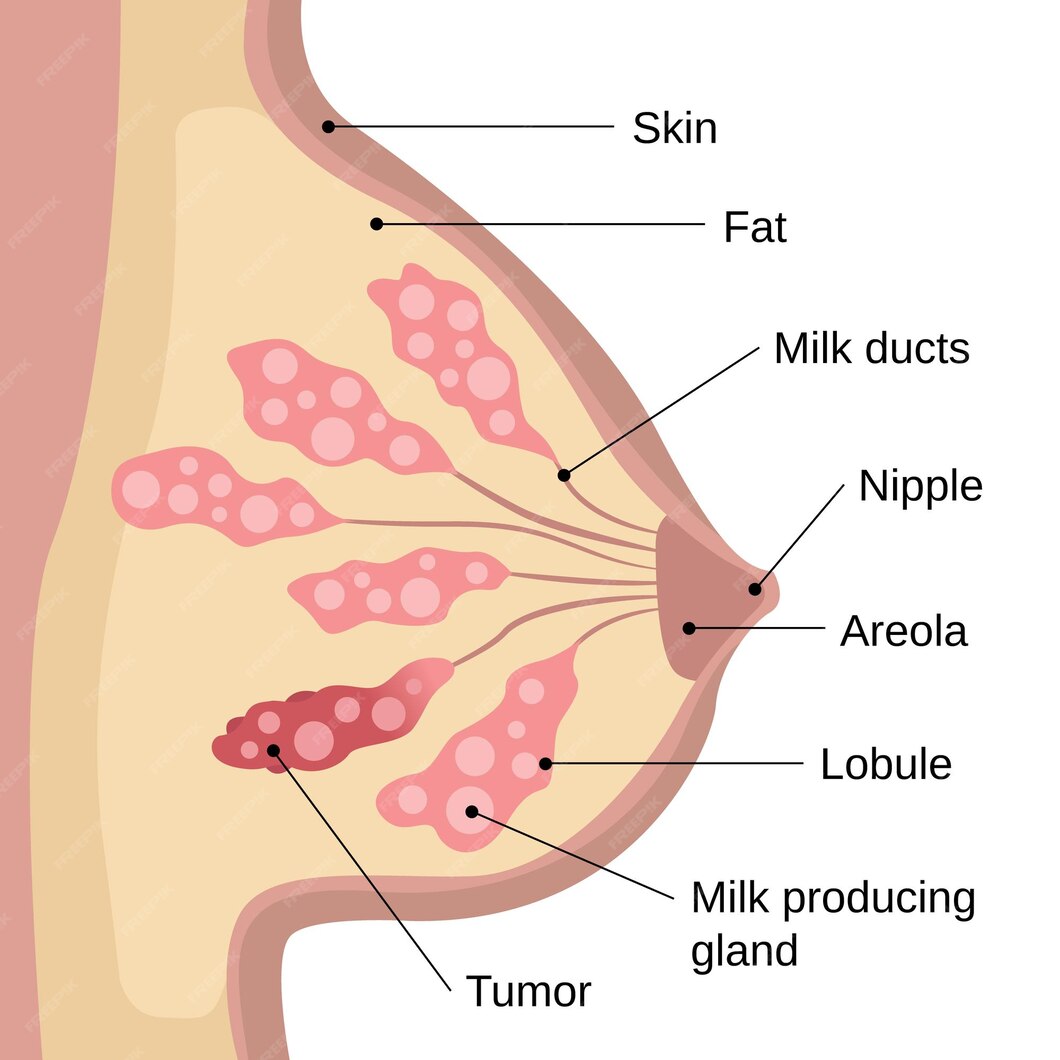
3. Breast Lump (e.g., Fibroadenoma, Cysts)
Description: Common benign breast lumps: fibroadenoma (young women) and simple cysts.
Presentation: Mobile, well-circumscribed, painless or tender; age and family history matter.
Investigations: Triple assessment — clinical exam, imaging (mammogram and/or ultrasound), and core biopsy or fine needle aspiration where indicated.
Treatment: Observation for benign lesions; ultrasound-guided aspiration for simple cysts; excision (lumpectomy) or core biopsy for indeterminate or symptomatic lesions.
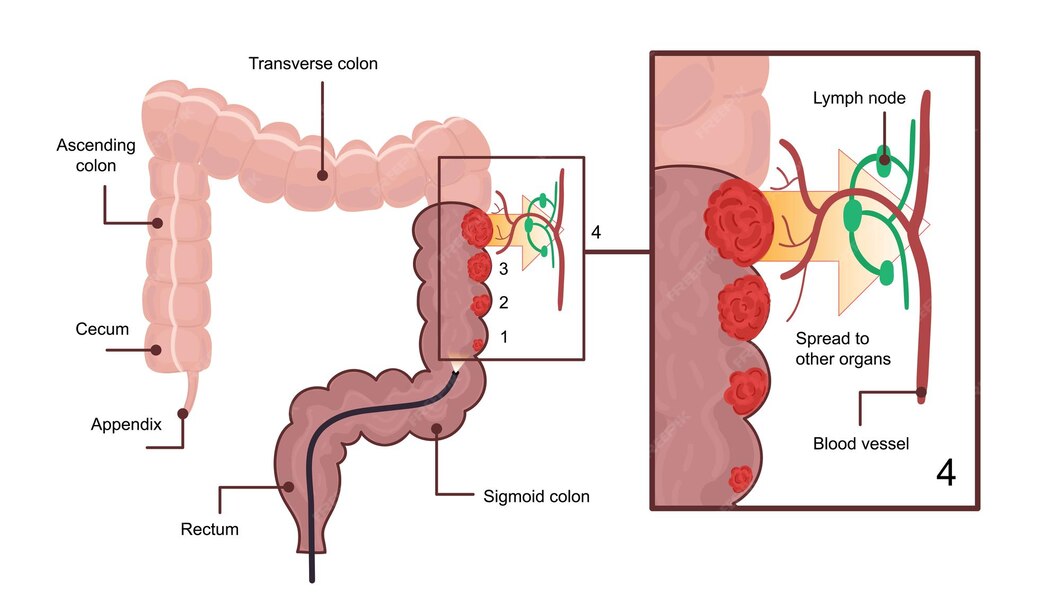
4. Enlarged Lymph Nodes
Description: Reactive lymphadenopathy is common; persistent, firm or rapidly growing nodes may indicate infection or malignancy. Presentation: Tender nodes often due to infection; hard, fixed, non-tender nodes raise concern. Investigations: Blood tests, ultrasound, fine needle aspiration cytology (FNAC) or core biopsy; targeted workup for infection or systemic disease. Treatment: Treat underlying infection when present; needle biopsy or excision biopsy for persistent or suspicious nodes; specialist referral if malignancy suspected.
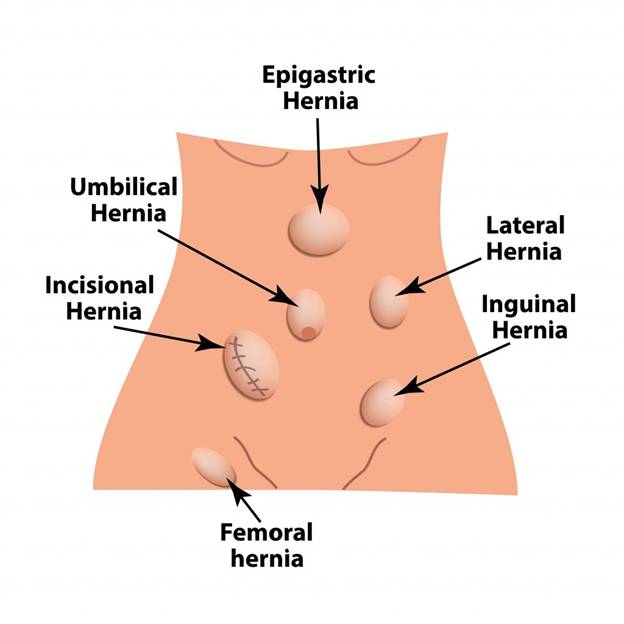
5. Hernia (Groin, Umbilical, Incisional)
Description: Protrusion of abdominal contents through a weakness in the abdominal wall. Presentation: Visible or palpable bulge, may be reducible, often worse with coughing or standing; pain or incarceration is urgent. Investigations: Clinical diagnosis; ultrasound or CT if uncertain. Treatment: Elective surgical repair for symptomatic or enlarging hernia; emergency surgery for incarcerated/strangulated hernia. Options include open or laparoscopic repair with or without mesh.
6. Ganglion Cyst
Description: Fluid-filled swelling commonly over wrist joints or tendon sheaths.
Presentation: Smooth, fluctuant lump that may change in size and cause mechanical symptoms. Investigations: Clinical assessment; ultrasound for confirmation. Treatment: Observation if asymptomatic; aspiration for symptomatic relief (high recurrence); surgical excision for persistent or recurrent ganglia.
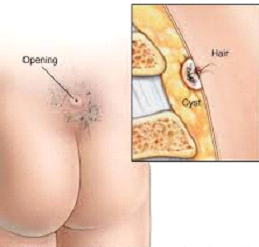
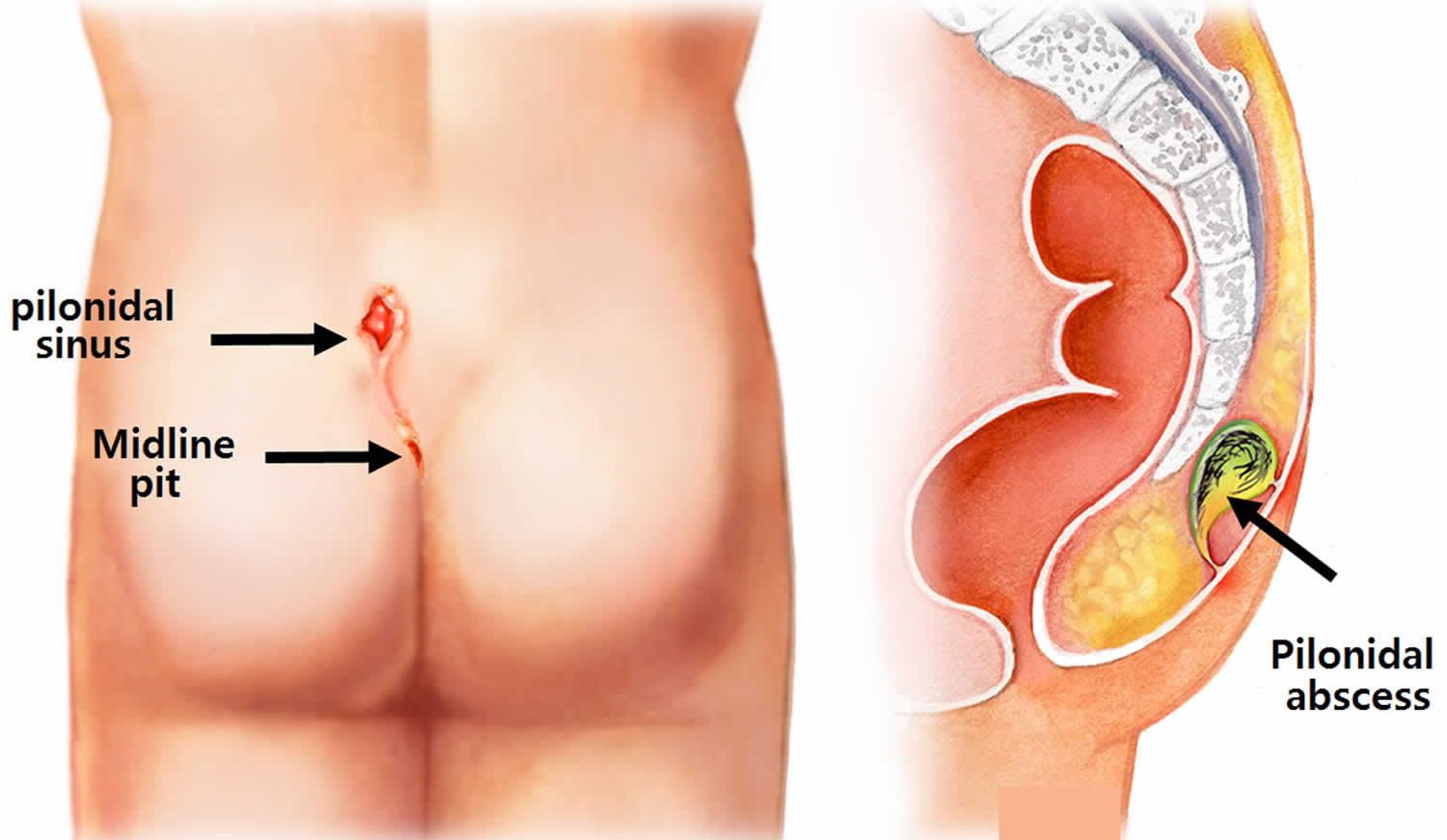
7. Pilonidal Sinus / Cyst
Description: A sinus/cyst near the natal cleft containing hair and debris; can form abscesses. Presentation: Painful swollen lump at the base of the spine with possible discharge. Investigations: Clinical diagnosis; ultrasound if complex. Treatment: Acute abscess — incision and drainage. Recurrent or chronic disease — excision of sinus with various closure techniques or off-midline flap procedures depending on severity. Emphasis on wound care and hair removal to prevent recurrence.
8. Dermatofibroma and Superficial Skin Lesions
Description: Small benign fibrous skin nodules (dermatofibroma) or cystic/vascular lesions. Presentation: Firm, small, often pigmented nodules on limbs; usually asymptomatic. Investigations: Clinical; dermoscopy; excision biopsy if uncertain. Treatment: Reassurance for benign lesions; surgical removal if symptomatic or for diagnosis.
9. Dermatofibroma and Superficial Skin
Description: Benign blood vessel growths present from infancy or acquired vascular lumps. Presentation: Red/blue compressible lesion; may bleed or be tender. Investigations: Clinical, ultrasound with Doppler; MRI for deeper lesions.
Treatment: Observation for small/asymptomatic lesions; compression, sclerotherapy, laser therapy or surgical excision depending on type and symptoms; multidisciplinary input for complex vascular anomalies.
10. Neurofibroma / Peripheral Nerve Tumors
Description: Benign nerve sheath tumors; multiple lesions may suggest neurofibromatosis. Presentation: Soft to firm lumps that may be tender or cause neurological symptoms. Investigations: Clinical exam, ultrasound, MRI, and biopsy when required. Treatment: Observation for small asymptomatic lesions; surgical excision if painful, growing, or causing functional impairment; referral to specialist centers for complex cases.
11. Suspicious or Malignant Masses (Red Flags)
Description: Any lump with rapid growth, hard/immobile texture, ulceration, or systemic ‘B’ symptoms. Action: Urgent imaging and tissue diagnosis (core biopsy or excision) and prompt referral to oncology or subspecialty surgery. Early diagnosis improves outcomes.
Investigations commonly used in OPD
Ultrasound (soft-tissue / Doppler) — first-line for many superficial lumps.
Fine-needle aspiration cytology (FNAC) — quick sampling for cytology.
Core needle biopsy — more tissue for histology when needed.
MRI / CT — for deep, large, or suspicious masses.
Blood tests / infection screen — when reactive or systemic disease suspected.
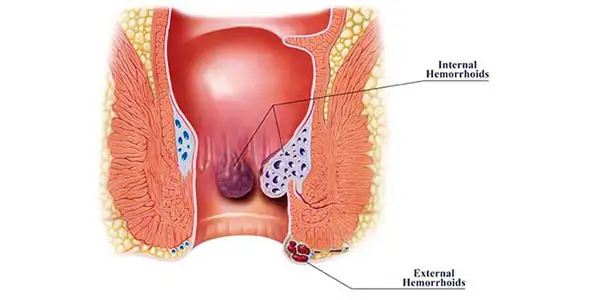
If you are experiencing symptoms of piles, or want to know which treatment is right for you, schedule a consultation with our colorectal specialists in Dubai.
Ground Floor - Villa No. 4 Al Wasl Rd - opposite Pizzahut - Jumeirah - Jumeirah 2 - Dubai
Address:
2nd of December Street 1st floor, Flat No 8, Al Satwa Bldg, Beside Civil, Defence, PO Box No 126590 - Dubai
Frequently Asked Questions (FAQs)
Which lumps are dangerous?
Red flags include rapid growth, hard/immobile mass, skin changes (ulceration or fixation), unexplained weight loss, and persistent enlarged nodes. These require urgent assessment.
Can lipomas turn into cancer?
True malignant transformation is rare; rapidly growing or very large lipomatous tumours are evaluated with imaging and biopsy to exclude liposarcoma.
Will cutting out a cyst leave a big scar?
Excision is done with skin-sparing techniques; scar size depends on lesion size and location. Elective excision after inflammation settles gives the best cosmetic outcome.
Are all breast lumps cancer?
No — many breast lumps are benign. However, all new breast lumps should be evaluated with imaging and, if needed, biopsy.
What is the recurrence risk after excision?
Recurrence depends on lesion type and completeness of excision (e.g., incomplete cyst wall removal increases recurrence for epidermoid cysts; ganglion cysts commonly recur after aspiration).